
Blocking GPVI on platelets with Glenzocimab
Monoclonal inhibitor shows promising results in randomised phase II

Before I go on, please follow my new podcast, Don’t Just Read the Abstract, available on all podcast platforms. We aim to critically appraise important studies in non-malignant haematology. The first trial we have looked at is the PACER trial, platelet transfusion prior to CVC insertion in patients who are thrombocytopaenic.
Glenzocimab
Being able to treat thrombosis without the causing bleeding is the holy grail of thrombosis research. It’s still unclear whether the two can be decoupled but a trial released this month shows a glimmer of hope.
Mazighi et al. reported results of ACTIMIS, a randomised, double-blind, placebo-controlled, phase 1b/2a trial in Lancet Neurology.
The trial took patients presenting with acute stroke who were receiving thrombolysis +/- mechanical thrombectomy. Investigators then administered 1000 mg glenzocimab, a monoclonal antibody fragment that blocks the platelet collagen receptor GPVI, or placebo.
The rationale for blocking GPVI is that it is a potent mediator of platelet activation but people with GPVI deficiency do not have a severe bleeding disorder - they have mild bleeding if any. Preclinical stroke models showed glenzocimab reduced infarct size and reduced ischaemia-reperfusion injury. Aside from it generally being quite interesting, this trial has peaked my interest as I work in a lab that has a lot of interest in GPVI biology as well as colleagues leading on a phase 2 trial of glenzocimab in STEMI.
The headline findings of the phase II part of ACTIMIS were:
106 patients randomised
Non-symptomatic haemorrhagic transformation
Glenzocimab: 17/54 (31%)
Placebo: 26/52 (50%)
Symptomatic intracranial haemorrhage
Glenzocimab: 0
Placebo: 5 (10%)
Complete recanalisation (mTICI score of 3) in those receiving mechanical thrombectomy
Glenzocimab: 12/27 (44%)
Placebo: 8/27 (30%)
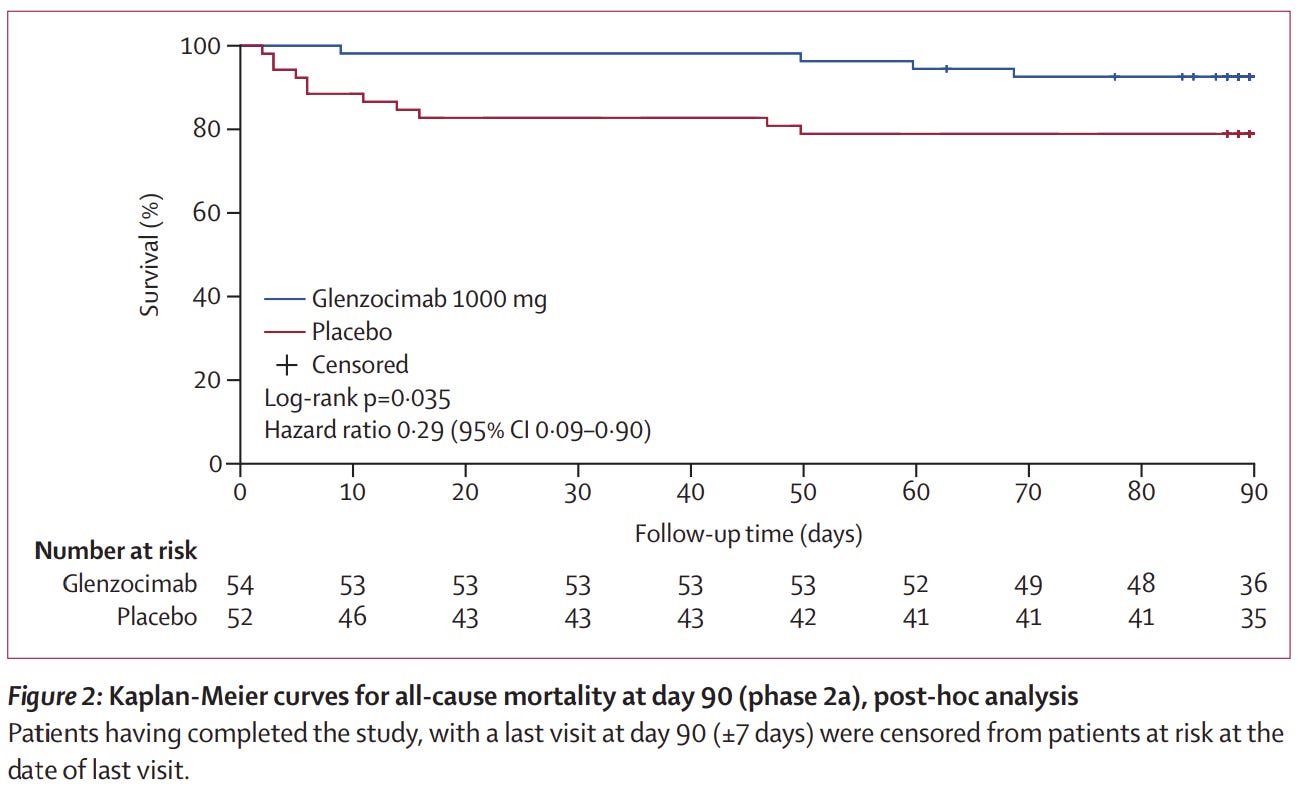
All-cause deaths lower with glenzocimab 1000 mg: 4 (7%) vs 11 (21%) patient. Overall survival benefit shown in Kaplan-Meier analysis.
They couldn’t look at infarct size due to lack of homogenous follow-up imaging.
The reduction in bleeding is striking. My colleague who is a glenzocimab expert thinks that this is probably due to reduction in infarct size - but this couldn’t be measured. However, the primary objective of a phase II trial is to show safety, which has been demonstrated in ACTIMIS. The main problem with interpretation is what to make of the reduction in bleeding and improvement in overall survival.
ACTIMIS lacks statistical power for efficacy
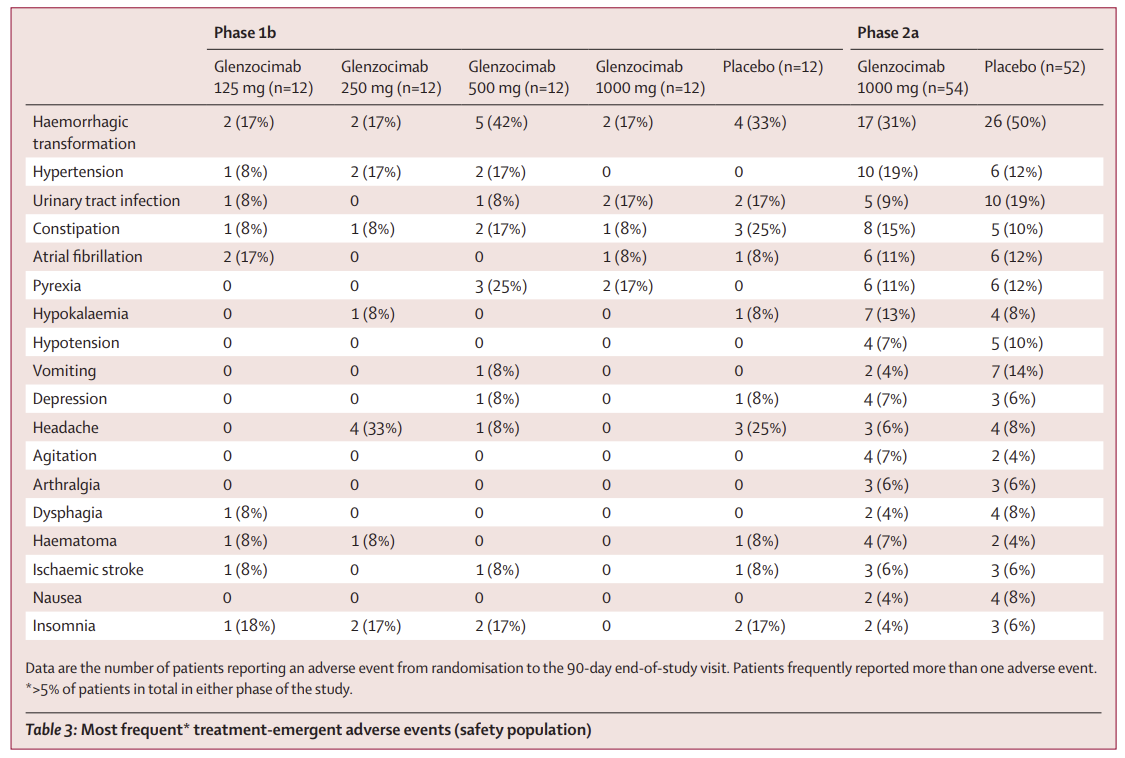
The first thing to say is that the study is underpowered for these efficacy end points. So, although there are statistically significant differences in bleeding and survival outcomes, the findings are not reliable. For example, look at table below, lifted from the paper. 7 (14%) patients who received placebo suffered vomiting vs. 2 (4%) patients who received glenzocimab. I can’t think of biological rationale for this - it’s almost certainly down to chance. If you measure enough things, you will find statistical differences - this is called multiplicity and this could also be the case for haemorrhagic transformation and overall survival.
It is well known that when studies with small sample sizes show beneficial effects of a treatment, the effect is often overestimated. Overall survival was also a post-hoc analysis and not a main aim of the study. The statistics behind all this are quite complex so you’ll have to just take it as read, but if you do want to read more, this article is quite useful.
Baseline differences in the groups might also be an explanation for the lower rates of haemorrhagic transformation in the glenzocimab arm - 0 patients in the glenzocimab arm had prior clopidogrel treatment compared to 5 in the placebo arm.
So, there is some hope here but the history of medicine tells us that many promising therapies ultimately fail to show benefit in larger studies. However, if glenzocimab does prove effective, it will be one of the first antithrombotic treatments that decouples treatment of thrombosis from adverse bleeding effects.
You can read more about the science of GPVI and glenzocimab here, in this lovely review from Gina Perrella who I have the pleasure of working with.